THE AUTHOR:

For pharmaceutical companies and contract research organizations seeking to build a pharmacovigilance automation platform, digitizing adverse event reporting is just the beginning of the challenge at hand.
The massive volume of global safety data is why the ICSR processing automation has been given top operational priority. As of February 2025, VigiBase, the World Health Organization’s database of medicines and vaccine safety, housed over 40 million reports from 180+ program member countries. Safety reports are submitted via email, PDF, patient programs, literature, partner systems, clinical trials, and regulatory databases. Each one must be validated, structured, coded, assessed, routed, and reviewed within strict time limits. Manual processing leads to long queues and inconsistent data, increases the cost of case management, and heightens the risk of compliance violations.
Regulatory infrastructure is also becoming more technical. Since April 1, 2026, commercial IND sponsors submitting ICSRs to the FDA’s AEMS through ESG NextGen have been required to use the ICH E2B(R3) standard.
Beginning October 1, 2026, the requirement will extend to all postmarketing ICSRs transmitted to AEMS through ESG NextGen. In the EU, EudraVigilance already requires ISO ICSR/ICH E2B(R3) messages and does not accept E2B(R2), making structured data models, XML validation, acknowledgement processing, and regulator-specific mapping central platform requirements.
Simultaneously, AI for pharmacovigilance is shifting from singular implementations to standard business practices. Deloitte’s 2026 Life Sciences Outlook indicates that 78% of responsible biopharma and medtech executives believe AI will be instrumental to large-scale organizational transformations. However, only 14% of executives reported full integration of AI into daily organizational workflows, meaning that gaps still exist with implementation, data, governance and process.
With that in mind, a modern automation solution for pharmacovigilance combines everything required to process drug safety cases in a controlled environment. This includes case intake, structured data extraction, duplicate case detection, coding, narrative writing, medical case reviews, regulatory submissions, audit trails and workload management. For contract research organizations (CROs) and pharma companies, this can have a significant impact on processing capabilities, compliance, costs of services, sponsor service level agreements (SLAs), and the ability to grow right-sized relative to case volume.
This article explains how to design the pharmacovigilance automation platform architecture, structure ICSR data, apply AI to appropriate processing tasks, integrate safety databases and regulatory gateways, validate automated components, and maintain accountable human review.
Selecting a development partner also requires evidence of regulated healthcare experience, integration capability, security controls, and production AI delivery.
Computools’ review of the top healthtech software development companies provides a broader comparison of providers working with healthcare platforms, clinical workflows, interoperability, AI, and protected data.
What should a modern pharmacovigilance automation platform control?
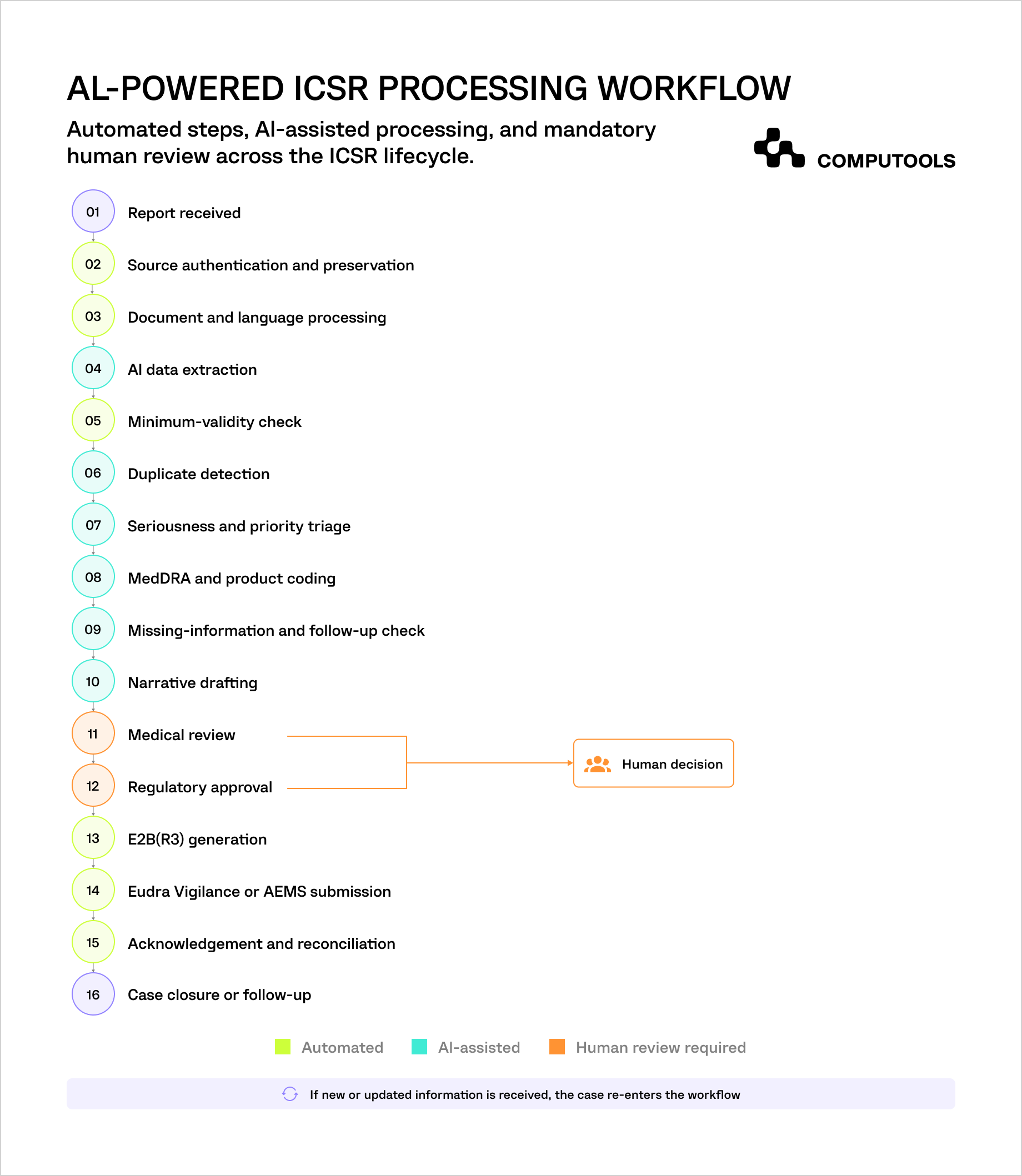
An ICSR case management software platform must coordinate the entire path from the first safety report to regulatory acknowledgement. The platform should divide the case lifecycle into controlled stages. Each stage needs defined inputs, validation rules, owners, approval boundaries, and measurable outcomes.
| Platform area | Primary responsibility | Human decision boundary | Operational KPI |
| Case intake | Capture reports from email, documents, portals, APIs, literature, and partner systems | Confirm unreadable, incomplete, or ambiguous source information | Time from receipt to case creation |
| Data structuring | Extract and normalise patient, reporter, product, event, and clinical details | Review low-confidence or conflicting values | Field acceptance and correction rate |
| Validation and triage | Check minimum case criteria, identify priority, and route work | Confirm potentially serious, special, or complex cases | Time to initial triage |
| Duplicate management | Compare new reports against existing and historical cases | Confirm whether records should be merged, linked, or retained separately | Duplicate-detection precision |
| Case processing | Support coding, follow-up, narrative creation, and quality checks | Approve terminology, narrative content, and case completeness | Processing time and rework rate |
| Medical review | Present evidence, discrepancies, and assessment recommendations | Make final seriousness, causality, expectedness, and reportability decisions | Reviewer override and return rate |
| Regulatory submission | Generate, validate, transmit, and reconcile E2B(R3) messages | Approve the final regulatory case | Submission rejection rate |
| Operational management | Track queues, deadlines, workload, exceptions, and sponsor SLAs | Reassign resources and manage escalations | SLA breach and backlog rate |
Automation depth should depend on the risk of each activity. Deterministic tasks, such as checking mandatory fields, calculating deadlines, validating XML schemas, and routing cases, can usually run automatically. Probabilistic tasks, including duplicate identification, coding recommendations, seriousness classification, and narrative preparation, should provide confidence scores and supporting evidence.
Final medical and regulatory decisions require stronger controls. The platform may prepare the information needed to assess causality or reportability, but it should not hide the source data, reasoning path, or changes made by reviewers. Every recommendation, correction, approval, and submission must remain traceable.
Computools case study: a scalable model for ICSR processing automation
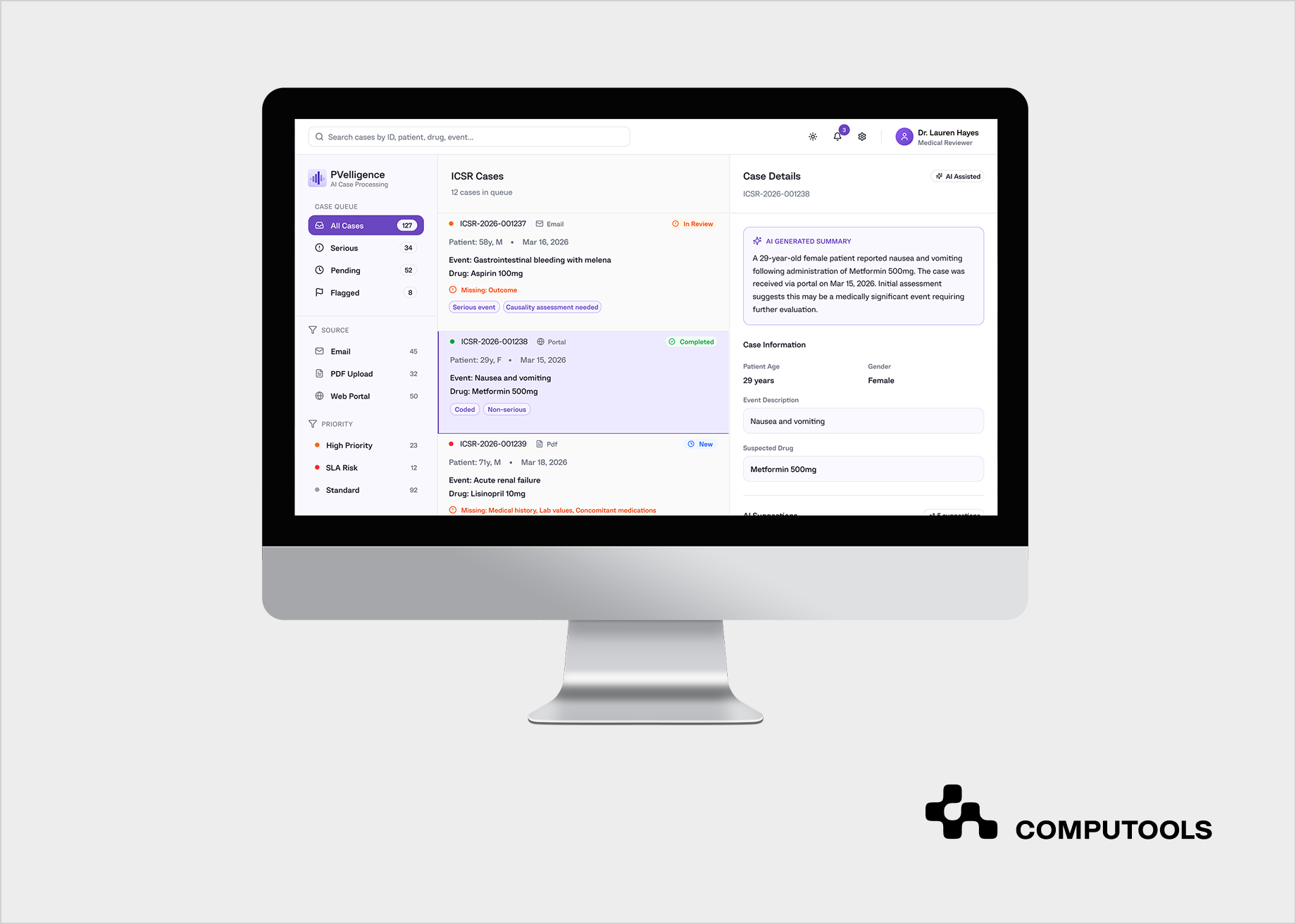
The operational value of automation becomes clearer when viewed through a high-volume pharmacovigilance environment. Computools developed PVelligence, an AI-powered platform for a contract research organisation that manages drug-safety operations for multiple life sciences sponsors.
Client Context
The CRO processed thousands of individual case safety reports each month. Cases arrived through monitored email accounts, PDF attachments, web portals, and other semi-structured sources. Each sponsor also followed its own standard operating procedures, reporting priorities, review requirements, and regulatory obligations.
This operating model created more complexity than a standard internal safety department faces. The platform had to support several client workflows while keeping sponsor data, rules, responsibilities, and deadlines clearly separated.
Business Challenge
The existing process depended heavily on manual work. Pharmacovigilance specialists had to transfer information from source documents, confirm case validity, structure patient and reporter data, map products through WHO Drug Dictionary terminology, assign MedDRA codes, prepare narratives, and enter approved information into safety systems.
For the CRO, this was a commercial as well as a compliance problem. Rising case volumes increased processing costs, placed more pressure on experienced reviewers, and limited the number of sponsor accounts the organisation could support without expanding its team at the same rate.
Computools Solution
Computools designed PVelligence around two connected layers: automated ICSR preparation and AI-assisted medical review.
The first layer deals with the collections of information and extracts specific safety pieces of information from unstructured documents. This layer then builds structured case records, checks a set of minimum validity standards, and aids in the triaging and coding of information. It drafts narratives and prepares information for regulatory processing. Natural language processing (NLP) and large language models (LLMs) help to identify key ICSR information elements.
These include the patient, the reporting individual, the suspect product, the reported adverse event, all relevant dates, and associated clinical information. Additionally, machine learning (ML) components help with the prioritization and classification of case seriousness, while robotic process automation (RPA) addresses case creation, and data population in case management and legacy systems, respectively.
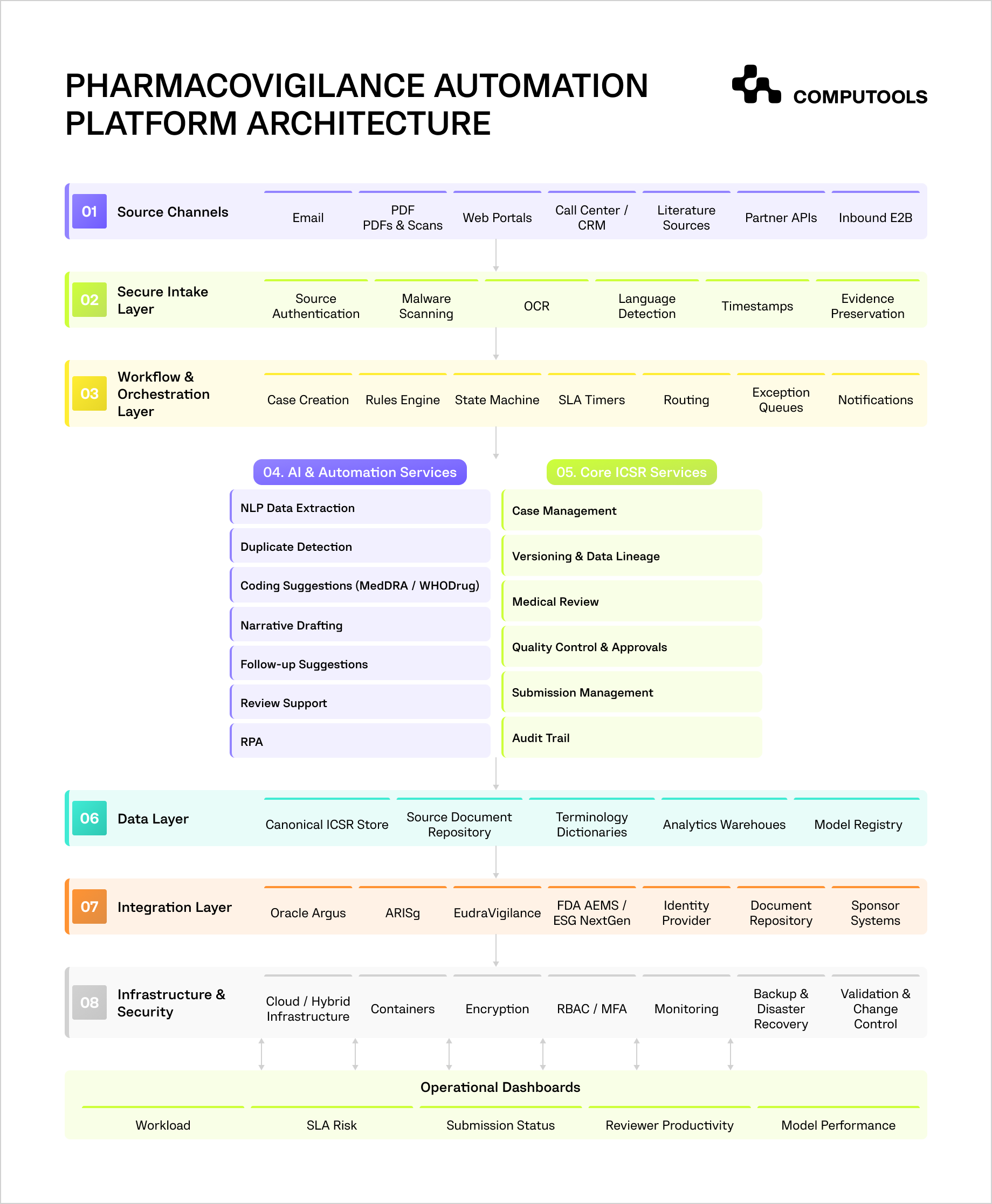
The entire system is based on the use of Python for orchestrating data pipelines, and integration with business logic. Upon such logic, TensorFlow and Keras are used for model development. An integration layer is used for data exchange with various pharmacovigilance systems, Oracle Argus and ARISg amongst them, along with email systems and document management. The safety of the systems is maintained with the use of AWS infrastructure, Docker, controlled role based access with the audit trails.
The second layer prepares cases for medical review. It presents seriousness, expectedness, causality, missing data, and reporting cues to physicians and pharmacovigilance specialists. The reviewer can verify, correct, or reject every recommendation. Clinically sensitive and regulatory decisions remain under human control rather than being submitted automatically.
Business Result
According to the project results, PVelligence reduced case preparation time from approximately four to six hours to 10–20 minutes before final human review. It automated up to 60–70% of the manual effort associated with intake, structuring, coding, and narrative preparation. The CRO also gained clearer visibility into workload, processing bottlenecks, and SLA exposure.
How to develop a pharmacovigilance automation platform
Effective pharmacovigilance software development involves working out the appropriate operating model prior to any AI capabilities. The software must be built around the way cases flow into the organization, which rules are applied, who/what is responsible for making the decisions, and how approved information is transferred to safety databases and the corresponding regulatory databases.
It is essential to determine which steps in the process are governed by fixed rules, which ones require medical judgment, where bottlenecks are located, and how case-specific requirements alter the process flow. These decisions will design the software architecture, the data model, the automation logic, and how software integrations and validations will be performed.
1. Define the Pharmacovigilance Operating Model
Capture how the organization manages cases across products, sponsors, jurisdictions, and reporting programs. A pharma company may have a single set of SOPs, while a CRO may operate several sets for different sponsors.
Define:
- supported intake sources and case types;
- postmarketing, clinical trial, and literature scope;
- countries and regulatory destinations;
- ownership of intake, triage, coding, medical review, quality control, and submission;
- sponsor-specific workflows and deadlines;
- points where automation must stop for human review.
These needs must be expressed in configurable workflows rather than custom-coded logic. The solution must be able to store routing rules, reporting timeframes, approval timeframes, escalation timeframes, and versions of SOPs as editable configurations.
One sponsor may need a medical review prior to the completion of the narrative, while another may require a quality-control stage post-coding. The workflow engine should be able to accommodate both cases.
The same applies for the logic for deadlines. The system should be able to establish due dates based on the receipt date, case type, level of seriousness, jurisdiction, and follow-up status. From a regulatory perspective, this should greatly ease the implementation of changes.
For multi-sponsor use, each tenant should have separate:
- users and permissions;
- workflows and SOP versions;
- product and reference data;
- dictionaries;
- reporting destinations;
- dashboards and SLA rules;
- audit and export access.
Shared services, such as document processing and AI inference, can support all tenants, but sponsor data must remain isolated.
The platform should also record which rule version applied to each case. When an SOP or regulatory requirement changes, open and historical cases may follow different logic. Without version control, teams cannot explain why a case took a specific route during an inspection.
In the PVelligence project, Computools separated repeatable ICSR processing from sponsor-specific review and approval rules. This allowed the platform to support multiple workflows while preserving clear permissions, responsibilities, and auditability.
Skipping this step usually leads to rigid software that fails when the organisation adds a sponsor, enters a new market, or updates an SOP. The result is manual workarounds, inconsistent routing, and repeated development effort.
2. Build a Controlled Multichannel Intake Layer
In life sciences pharmacovigilance software, safety reports may arrive through monitored email, PDFs, web forms, call centres, partner portals, literature sources, APIs, or inbound E2B messages. The team should decide which channels can create a case automatically and which require intake confirmation.
The intake layer should:
- authenticate the source where possible;
- scan files for malware;
- detect language and document type;
- preserve the original report;
- record receipt date and time;
- extract text and metadata;
- assign a unique source identifier;
- route unreadable or incomplete reports to an exception queue.
Each extracted value should remain linked to its source page, paragraph, attachment, or message. Reviewers must be able to compare structured data with the original evidence without searching through several systems.
The platform should also separate source data from processed data. For example, the original product name should remain unchanged, while a normalised product value and dictionary code are stored as separate fields. The same rule applies to dates, medical terms, reporter statements, and AI-generated content.
Technical recommendation: Use an event-driven intake pipeline in which every new report creates a processing event rather than triggering one long synchronous request. Separate file storage, OCR, language detection, extraction, validation, and case creation into independent services connected through a message queue. This allows failed tasks to be retried without processing the entire report again and prevents large attachments or slow OCR jobs from blocking other cases.
In PVelligence, Computools used a single intake layer for email, PDFs, forms, and other semi-structured sources. The platform converted them into consistent case records before coding and review.
In adverse event reporting, weak intake controls create missing evidence, duplicate records, incorrect receipt dates, and unclear audit histories. These problems become harder to correct after the case enters the main safety database.
3. Design a Canonical ICSR Data Model
The AI-powered drug safety platform needs one internal data structure that can support different sponsors, safety databases, and regulatory destinations. Building the database directly around one external XML format creates rigid mapping logic and makes future changes expensive.
The data model should cover:
- patient and reporter details;
- suspect, interacting, and concomitant products;
- adverse events;
- dosage and treatment dates;
- medical history;
- laboratory results;
- seriousness criteria;
- outcomes;
- narratives;
- source references;
- follow-up information;
- submission and acknowledgement history.
For each field, store the original value, extracted value, normalised value, coded value, confidence score, and approved value where relevant. This preserves data lineage and shows how the record changed during processing.
The platform should also support case versions. A follow-up report should update the same case history without overwriting the original submission. Reviewers need to see what changed, who approved it, and whether the new information affects seriousness, expectedness, or reportability.
The regulatory mapping layer should convert approved internal data into E2B(R3) messages. It should handle controlled terminology, required fields, null values, XML schema validation, destination-specific rules, and acknowledgement responses.
Technical recommendation: Use an immutable versioning model for safety cases rather than updating records in place. Store every approved change as a new case version with links to the previous version, source evidence, reviewer, rule set, and timestamp. Keep E2B(R3) mapping in a separate adapter layer so regulatory format changes do not require changes to the core database schema.
Without a canonical model, integrations often create conflicting versions of the same case. Teams then spend time reconciling data instead of reviewing safety information.
4. Automate Validation, Triage, Routing, and Deadlines
Pharmacovigilance workflow automation should combine deterministic rules with AI-based recommendations. Fixed rules control tasks where the correct result can be defined clearly. AI supports tasks that depend on patterns, context, or probability.
Use deterministic logic for:
- minimum case-validity checks;
- mandatory-field validation;
- reporting deadline calculation;
- jurisdiction and sponsor routing;
- escalation;
- workflow transitions;
- submission readiness;
- quality-control requirements.
Use AI or similarity models for:
- possible duplicate detection;
- seriousness candidate classification;
- priority scoring;
- likely missing-information identification;
- workload and SLA risk prediction.
The workflow engine must track the case details, case state, owner, priority, and deadline, as well as retry, exception, and escalation pathways. The engine must block users from skipping required review stages, and from approving a case if required information has not been provided.
Avoid allowing an AI model to control final reportability or submission deadlines. These decisions should remain tied to approved rules and qualified review.
Technical recommendation: The workflow must be explicitly modeled as a state machine with controlled states of Received, Validated, In Processing, Medical Review, Quality Control, Ready for Submission, Submitted, and Closed. Deadline calculation must be kept as separate, versioned rules, with background workers controlling deadlines and triggering escalations. This is more reliable than checking deadlines only when a user opens a case.
Poor workflow design causes hidden backlogs, missed handoffs, and cases that appear active without a clear owner. A well-designed engine makes every delay and exception visible.
5. Add AI to High-Volume Preparation Tasks
AI works best in case processing automation in pharmacovigilance when it reduces repetitive preparation without replacing accountable medical decisions. The team must state which outputs can be accepted without manual intervention, which must be reviewed, and which will be treated as recommendations.
The following pharmacovigilance AI solutions can be of assistance:
| Capability | Description |
| Structured data extraction | Pulls out information on patients, reporters, products, as well as event reporting and related history from unstructured reports. |
| Coding suggestions | Provides suggestions for MedDRA term/class coding and product coding based on context and language of the reporting or record. |
| Duplicate detection | Compares patient details, products, events, dates, source metadata, and narrative similarity. |
| Narrative drafting | Creates a first draft from approved structured fields and source evidence. |
| Medical-review support | Surfaces seriousness indicators, missing data, expectedness references, and possible inconsistencies. |
| Follow-up assistance | Recommends questions based on missing clinical or reporting information. |
| Approved-content search | Allows reviewers to search SOPs, reference safety information, product labels, and regulatory guidance through controlled retrieval. |
| Operational prediction | Identifies cases at risk of missing internal or regulatory deadlines. |
Each AI output should include a confidence score, source reference, model version, and reviewer action. The system should record whether the reviewer accepted, edited, or rejected the result. These corrections can support controlled model improvement.
Clean, structured data is essential. Historical cases with inconsistent labels, incomplete coding, or unclear corrections will produce unreliable models.
The training and testing data should contain multilingual cases, reports for rare events, and complex cases as well as sponsor specific terminology.
Technical recommendation: In order to support the different functionalities of extraction, terminology checking, duplicate case identification and narrative generation, use separate models or services rather than a single model that encompasses all of these features. Apply confidence thresholds by field and risk level. A low-confidence treatment date may enter a review queue, while a low-confidence seriousness indicator should trigger mandatory specialist review. Ground generated narratives only in approved case fields and source passages to reduce unsupported content.
PVelligence uses AI to prepare structured records, coding suggestions, narratives, and review cues. Final clinical and regulatory decisions remain with pharmacovigilance specialists.
A model with strong overall accuracy may still fail on rare but high-risk cases. Teams should therefore measure performance by field, case type, language, and seriousness category rather than relying on one general score.
The same engineering principles apply to other regulated workflows that convert unstructured medical records into structured information.
Computools’ guide on how to build an AI system for clinical documentation explains how medical NLP, standardized data pipelines, role-based review, and secure storage support accurate automation without removing professional control.
6. Connect Safety Databases and Regulatory Gateways
Most organisations do not replace their validated safety database immediately. They add an automation and orchestration layer that exchanges approved information with systems such as Oracle Argus, ARISg, document repositories, regulatory gateways, and sponsor portals.
The integration architecture may use:
- REST or vendor APIs;
- E2B(R3) XML;
- secure file transfer;
- message queues;
- scheduled synchronisation;
- controlled RPA where no API exists.
Each integration should support validation, retries, reconciliation, duplicate protection, and failure recovery.
For regulatory submissions, the platform should record:
- message version;
- destination;
- transmission time;
- acknowledgement;
- validation status;
- rejection reason;
- correction and resubmission history.
Employ idempotency controls to avoid duplicate case creation or submissions. Messages that fail to process should go to a dead-letter queue for analysis, rather than disappearing without notice.
Controlled synchronization is also essential for reference data. MedDRA versions, product dictionaries, sponsor lists, user roles, and reporting destinations should be updated under a defined process with an explicit effective date.
Technical recommendation: Each external system should be separated by a dedicated integration adapter. Each of these should have its own configuration for mapping, authentication, retries, and reconciliation. Use correlational IDs for every submission to allow a full trace of the case. Store outbound messages and regulator responses as immutable records rather than relying only on external system logs.
In PVelligence, Computools connected the automation layer with Argus, ARISg, email services, and document storage. RPA supported repetitive entry where direct interfaces were limited.
A technically successful case workflow can still fail if the final message never reaches the regulator or acknowledgement errors remain unresolved. Integration monitoring should therefore be part of the operational dashboard, not a separate IT log.
For systems processing U.S. healthcare data, the architecture should also account for HIPAA-related privacy and security requirements where applicable. For more information, check the Computools guide to designing HIPAA-compliant AI architecture.
7. Protect Case Data and Preserve Auditability
A regulatory compliance software for pharmacovigilance must protect patient, reporter, product, sponsor, and clinical information throughout the entire case lifecycle.
Core controls should include:
- role-based and attribute-based access;
- multi factor authentication;
- tenant separation;
- encryption in transit and at rest;
- secrets and key management;
- immutable audit records;
- session monitoring;
- data-retention rules;
- regional storage controls;
- tested backups and recovery procedures.
Every meaningful action should be traceable. The audit history should show who viewed, edited, coded, reviewed, approved, exported, or submitted a case. It should also record workflow changes, rule versions, AI outputs, reviewer corrections, and integration failures.
AI introduces additional risks. Case data should not be sent to public model services or reused for training without an approved data-processing arrangement. The architecture should support controlled model endpoints, private networking, output logging, model-version tracking, source grounding, and manual fallback.
Tenant separation is especially important for CROs. Sponsor A must never be able to access Sponsor B’s cases, product information, metrics, or model context. Shared processing services should use strict access controls and isolated data paths.
Technical recommendation: Apply zero-trust access at both the user and service level. Use short-lived credentials, service identities, private network endpoints, and centralised secrets management. Keep audit events in append-only storage with retention controls, and test tenant isolation through automated security tests that attempt cross-sponsor access at the API, database, search, cache, and analytics layers.
Cloud deployment requires consistent protection across storage, processing, AI inference, APIs, and connected safety systems. Computools’ article on cloud security in healthcare businesses covers key practical controls.
8. Validate the Platform and Improve It After Launch
Validation of drug safety software solutions should reflect intended use and risk. A mandatory-field rule, narrative model, duplicate detector, and regulatory submission service should not receive the same testing approach.
Workflow testing should cover:
- permissions and role separation;
- required review stages;
- deadline calculation;
- escalations;
- case versioning;
- follow-up processing;
- approvals and electronic records.
Regulatory testing should verify:
- E2B(R3) message generation;
- schema and business-rule validation;
- controlled terminology;
- acknowledgement handling;
- rejection recovery;
- resubmission;
- reconciliation with the target safety database.
AI testing should measure:
- field-level extraction precision and recall;
- coding acceptance;
- duplicate-detection performance;
- narrative accuracy;
- unsupported statements;
- multilingual performance;
- false negatives in serious cases;
- consistency after model, prompt, or data changes.
Performance testing should simulate peak intake, large attachments, batch processing, unavailable external systems, queue recovery, and partial integration failures. Testing only normal daily volume may hide bottlenecks that appear during product launches, safety alerts, or large literature imports.
After launch, monitor:
- receipt-to-case-creation time;
- time to ready-for-review;
- field correction rates;
- reviewer overrides;
- rework;
- duplicate confirmation;
- SLA breaches;
- submission rejections;
- acknowledgement delays;
- cost per case;
- reviewer capacity;
- model drift.
Measure automation by task rather than using one platform-wide percentage. A system may automate most document extraction while still requiring extensive manual correction in coding or narrative preparation.
Launch your AI-powered ICSR automation platform within 1–3 months instead of years, and give your pharmacovigilance team the capacity to handle growing case volumes without growing operational costs.
Why choose Computools for pharmacovigilance automation platform development
Computools designs pharmacovigilance platforms to address operational problems that increase case costs, slow reporting, and limit growth. These include fragmented intake channels, repetitive data entry, inconsistent sponsor workflows, weak deadline visibility, difficult safety-database integrations, and excessive reviewer time spent on preparation rather than medical assessment.
Our team connects case intake, AI-assisted processing, reviewer workflows, regulatory submissions, sponsor rules, analytics, and existing safety systems within one controlled architecture.
Our healthcare software development services support secure clinical workflows, protected health data, controlled access, and inspection-ready records. Pharmaceutical software development services address sponsor-specific SOPs, drug-safety processes, regulatory reporting, and product-level rules.
Through data engineering, our team builds canonical ICSR models, traceable data pipelines, terminology mappings, source-to-field lineage, and E2B(R3) transformation logic. This reduces reconciliation work and prevents conflicting case versions across intake tools, safety databases, and regulatory outputs.
Our AI development expertise supports structured extraction, duplicate detection, coding recommendations, narrative drafting, review assistance, confidence thresholds, and model monitoring. AI outputs remain connected to source evidence and reviewer actions, which reduces unsupported recommendations and protects professional accountability.
Computools also applies web development services to create focused workspaces for intake teams, case processors, medical reviewers, quality specialists, administrators, and sponsor managers. These interfaces reduce unnecessary handoffs by bringing source evidence, case data, exceptions, approvals, deadlines, and workload indicators into one operational view.
The PVelligence project demonstrates practical experience with high-volume ICSR processing, NLP-based data extraction, coding support, narrative preparation, medical-review assistance, RPA, and integrations with systems such as Oracle Argus and ARISg. According to the project results, case preparation time fell from four to six hours to 10–20 minutes before final review, while 60–70% of manual processing effort was automated.
With 250+ engineers, 400+ delivered projects, ISO 9001 and ISO 27001 certifications, and AWS and Microsoft partner expertise, Computools can support both initial delivery and long-term platform development.
Our clients receive a connected pharmacovigilance operating platform that reduces case-processing costs, protects reporting continuity, improves reviewer productivity, strengthens sponsor service, and creates capacity for further growth.
Final thoughts
Consider an AI-driven pharmacovigilance automation platform, an operational control system rather than a standalone AI interface or document processing system. The value of the platform lies in the integration of intake channels, structured ICSR data, workflow, and medical review, regulatory submissions and controls, sponsor and audit submission requirements.
The strongest advantages come from the elimination of manual preparation for reporting, reduction of review time, clearer visibility of deadlines, and increased capacity to process submissions. Achieving this with pharmacovigilance case intake automation will require a controlled integration, safe and secure cloud framework, validated workflows, and measurable traced performance post validation with the AI embedded in the platform.
Companies should keep focusing on building an operational control system. AI can extract, classify, provide, and prepare recommendations, while qualified specialists are accountable to provide the medical review and approve the final report.
Computools
Software Solutions
Computools is an IT consulting and software development company that delivers innovative solutions to help businesses unlock tomorrow.






